






This article explores how stigma impacts healthcare for people with learning disabilities and how nurses can improve the patient experience and outcome through inclusive practice. This is a Journal Club article and comes with a handout that you can download and distribute for a journal club discussion.
The NT Journal Club offers an opportunity to reflect on practice, share insights and ideas in a relaxed and sociable setting, and gain participatory CPD hours towards revalidation. Click here to find out about the NT Journal Club and for more journal club articles to discuss.
Abstract
A significant history of stigmatisation towards people with learning disabilities has resulted in serious healthcare inequalities for this population, affecting access to testing, screening and monitoring, and appropriate inpatient care. However, despite evidence highlighting these disparities – including discriminatory practices during the Covid-19 pandemic – little progress has been made in addressing them. Research identifies indifference towards individuals with intellectual disabilities as a key factor in these disparities. This article, the second in the series on stigmatisation in healthcare, briefly explores the stigma of intellectual disabilities in the context of equality, diversity and inclusion in healthcare, and proposes strategies to address such discrimination that leads to poor practice.
Citation: Blair J, Porter S (2025) Supporting nurses to understand and address stigma towards people with learning disabilities. Nursing Times [online]; 121: 8.
Author: Joanne Blair and Dr Shannon Porter are both lecturers (education), Queen’s University Belfast.
Introduction
The word ‘stigma’ refers to unfair negative beliefs held about someone or something. It is important to acknowledge that stigma can present as an unconscious bias – that is, an assumption of which someone is not consciously aware (Oxtoby, 2020). In the context of stigma towards people with learning disabilities (LD), it is first essential to define the meaning of LD.
In the 11th edition of the International Classification of Diseases, the World Health Organization (WHO) (2025) defines LD under the umbrella term of ‘disorders of intellectual development’. These are described under Code 6A00 as “a group of etiologically diverse conditions originating during the developmental period, characterised by significantly below-average intellectual functioning and adaptive behaviour that are approximately two or more standard deviations below the mean… based on appropriately normed, individually administered standardised tests”. Mencap (no date a) explain it more simply as a reduced intellectual ability and difficulty carrying out everyday tasks and activities, which will affect the individual for the whole of their life.
Mencap (no date c) suggests that ~1.5 million people in the UK have LD. When family, loved ones, carers and healthcare workers are considered, there are a significant number of people who are impacted by stigma and the resulting health inequalities experienced by this population.
A historical perspective
Stigma towards individuals with LD has been deeply ingrained in societal perceptions and practices throughout history. Over time, people with LD have faced significant challenges due to misconceptions and negative attitudes. Stigmatisation often stems from the belief that individuals with disabilities are less capable of contributing to their families and communities, leading to the perception that they are burdensome (Oguntayo et al, 2020). This expectation of lower abilities and productivity has perpetuated stereotypes and discrimination against individuals with LD.
Historically, individuals with LD have not only been categorised based on their disability, but have also faced additional stigma – such as being labelled unfit to live an ordinary life or participate actively in society (Scior and Werner, 2015). This added layer of stigma has contributed to the perpetuation of myths and negative perceptions about LD. Studies have shown that significant levels of stigma exist towards people with LD – not only from the general community, but also from caregivers and professionals working with individuals who have disabilities (Pelleboer-Gunnink et al, 2017).
The impact of historical stigma on individuals with LD has been profound, affecting various aspects of their lives. Stigmatisation can manifest in direct forms, such as physical and verbal abuse, as well as more subtle forms of disempowerment (Haft et al, 2023). Individuals with LD are vulnerable to experiences of stigmatisation, which can have detrimental effects on their academic performance and emotional wellbeing (Richards et al, 2019).
Recent evidence highlights how the Covid-19 pandemic has exacerbated stigma towards individuals who have LD, with Scherer et al (2023) revealing that inaccessible Covid-19 information, delayed vaccination priority and limited care guidance all increased vulnerabilities for individuals with LD, thereby having a negative effect on their wellbeing and quality of life.
The historical context of exclusion and discrimination against individuals with disabilities has contributed to the perpetuation of negative stereotypes and societal attitudes. Efforts to address the historical stigma towards individuals with LD have been ongoing, with initiatives aimed at challenging misconceptions and promoting inclusivity.
Research has highlighted the importance of creating positive images and narratives of people with intellectual disabilities to combat stigma and discrimination (Daley and Rappolt-Schlichtmann, 2018). Although there has been a progressive move to community living and integration, there is still significant work to be done to reduce the stigma attached to people with LD. Understanding the historical context of stigma towards individuals with LD is crucial for developing strategies to promote acceptance, equality and empowerment for them.
Impact of stigma
People with LD are living for longer compared with previous generations (Foundation for People with Learning Disabilities, no date), but Glover et al (2020) pointed out that this does not mean that they are living heathier lives. Premature death among people with LD has been a topic of discussion for many years. Males with LD die, on average, 13 years sooner than those in the general population, and females ~20 years earlier (Heslop et al, 2014).
Specific disparities have been noted over the years. Hughes-McCormack et al (2018) identified that children with LD were more likely to have poorer health and poorer experiences of healthcare than those without LD. Nicholson et al (2022) reported that, despite these children having a higher incidence of chronic conditions, this was not demonstrated through increased visits to either the GP or to the emergency department.
Carey et al (2016) stated that, compared with the general population, people with LD are more likely to have chronic conditions such as epilepsy, mental health problems and dementia, as well as other physical health conditions such as diabetes, constipation and hypothyroidism. Ailey et al (2015) identified that admission rates to general hospitals were up to 1.6 times greater for people with LD compared with people in mainstream populations.
“Educational interventions can be a useful strategy to reduce stigma”
Importantly, Williamson et al (2021) highlighted the higher risk of hospital admission and death due to Covid-19 for all groups with LD when compared with the general population. This emphasised that there were nurses working in pri-mary and acute environments who were routinely caring for people with LD, yet evidence clearly highlighted the ongoing lack of equality in healthcare for people with LD.
People with LD are more likely to have a disease, or symptoms of a disease, and higher rates of medical complexity than people in the general population; in addition, the onset of disease appears to happen much earlier than in the general population but is more likely to go undiagnosed (Chapman et al, 2018). This is suggested to be the result of ongoing challenges for people with intellectual disabilities when trying to access the healthcare they need (Chapman et al, 2018).
The move from institutions to community-based living – and, thus, from a medical to a social model of care – has done little to challenge negative and discriminatory attitudes towards people with LD (Shakespeare et al, 2017). McCarron et al (2015) highlighted the complexity of health and healthcare for people with LD compared with the mainstream population, and the challenge for services to deliver the person-centred care that is needed. When this is explored alongside the challenges people with LD face trying to access the health service they need, it becomes apparent why this inequality exists (Chapman et al, 2018).
Research continues to highlight multiple barriers faced by people with LD when trying to access the health and social care they need, as compared with those without disabilities. This was evidenced many years ago in two Mencap reports, published in 2007 and 2012, which suggested that “institutional discrimination” was the reason for it. A case study from the later report is included in Box 1 to support practice reflection. The point was also evidenced more recently, in the Confidential Inquiry into Premature Deaths of People with Learning Disabilities (CIPOLD) (Heslop et al, 2014), which supported Mencap’s findings. These reports all raise concerns about the stigma attached to having LD.
Box 1. Insititutional discrimination: practice reflection exercise
The following case study was published in Mencap’s Death by Indifference: 74 Years and Counting report:
“Christopher Peters was a fun-loving young man who was a fan of Michael Jackson and a much-loved member of his [own] family. Christopher was admitted to Aintree Hospital on the evening of 25 February 2009 with severe abdominal pain. Despite a rapid deterioration in his condition, Christopher was not operated on until 4am the following day and tragically died soon afterwards of small bowel ischaemia and septic shock. The family consider that, had Christopher been operated on soon after admission, he would at least have had a chance of survival.
“Christopher’s family were with him throughout those agonising hours in hospital. For most of this time, Christopher was in terrible pain, but despite his mother Wendy’s constant pleas to the ward staff to get relief for her son’s pain, it took almost two hours for any of the surgical team to attend. By this time, Christopher’s abdomen had extended to ‘the size of a football’ and he was bleeding profusely. Subsequently, Christopher’s hospital records were found to contain comments, including one that said: ‘this gentleman did not get the care and attention he deserved’.”
Reflect on your own attitude to people with learning disabilities.
How would you respond to Christopher’s family’s concerns?
Adapted from Mencap (2012)
Stigma in the care of people with LD is well known and new evidence continues to emerge, yet on a practical level little appears to have changed in response. The CIPOLD identified a number of factors as contributing to the premature death of people with LD, including:
- Problems with advanced care planning;
- Lack of adherence to the Mental Capacity Act 2005;
- Inappropriate living arrangements;
- Carers not being listened to;
- A reluctance to adjust care according to changing needs (Heslop et al, 2014).
For people with LD, diagnostic overshadowing – the misattribution of symptoms of physical or mental illness to an individual’s existing condition – has led to delays in assessment, diagnosis and treatment and, in some cases, death (Heslop et al, 2014). White et al’s (2023) report – namely, LeDeR: Learning from Lives and Deaths: People with a Learning Disability and Autistic People 2022 – highlighted the importance of this following concerns that sepsis had been missed in an individual with LD, due to diagnostic overshadowing, and that sepsis guidelines were not adhered to.
Recent news coverage of the preventable death of 11-year-old Mattheus Vieira, a non-verbal child with autism, has put this issue firmly under the spotlight, with his death being determined as neglect and a failure in care (Lynn News, 2024).
To avoid diagnostic overshadowing, simple strategies can be put in place – these have been outlined in Box 2.
Box 2. Strategies to prevent diagnostic overshadowing
- Approach your assessment as you would for anyone else – namely, see the individual
- Consider their communication needs and ask how you can best meet these
- Involve family/carers – they are your best source of information aside from the individual themselves
- Remember, quality of life is subjective; people do not suffer from learning disabilities
- Use available resources to help in your assessment, such as:
- The Distress and Discomfort Assessment Tool – for pain assessment in those with limited or no verbal communication
- The HSC Hospital Passport – helps provide valuable information about the person with learning disabilities
- Listen to the people who know the individual best; they are the experts
Addressing the stigma of LD in healthcare
Much is being done in practice to better meet the needs of people with LD. The NHS’s (2019) NHS Long Term Plan was developed with this in mind and aimed to improve services and close the gap in healthcare for people with LD in England. There is evidence to suggest this has had some impact, with White et al’s (2023) LeDeR report indicating a slight drop in avoidable deaths in this population and a small increase in life expectancy. This report also indicated, however, that much work was still needed. There is no quick fix to addressing stigma in healthcare, but a good starting point is giving consideration to:
- Reasonable adjustments;
- Person-centred care;
- Communication;
- Capacity legislation and best interests;
- Education about LD.
Reasonable adjustments
The Equality Act 2010 states that anyone who provides a service to the public must make reasonable adjustments for people with disabilities and, in healthcare, this is applied as a means of addressing unnecessary barriers to accessing care. Key barriers have been identified as:
- Communication difficulties (Tuffrey-Wijne et al, 2014; Tuffrey-Wijne et al, 2013);
- Poor access/provision of health promotion and screening (Sakellariou and Rotarou, 2017);
- Poor attitudes of staff caring for individuals with LD (Tuffrey-Wijne et al, 2014; Tuffrey-Wijne et al, 2013).
Table 1 highlights examples of reasonable adjustments that are straightforward to implement in practice, yet contribute greatly to improve patient experience and health outcomes for people with LD.
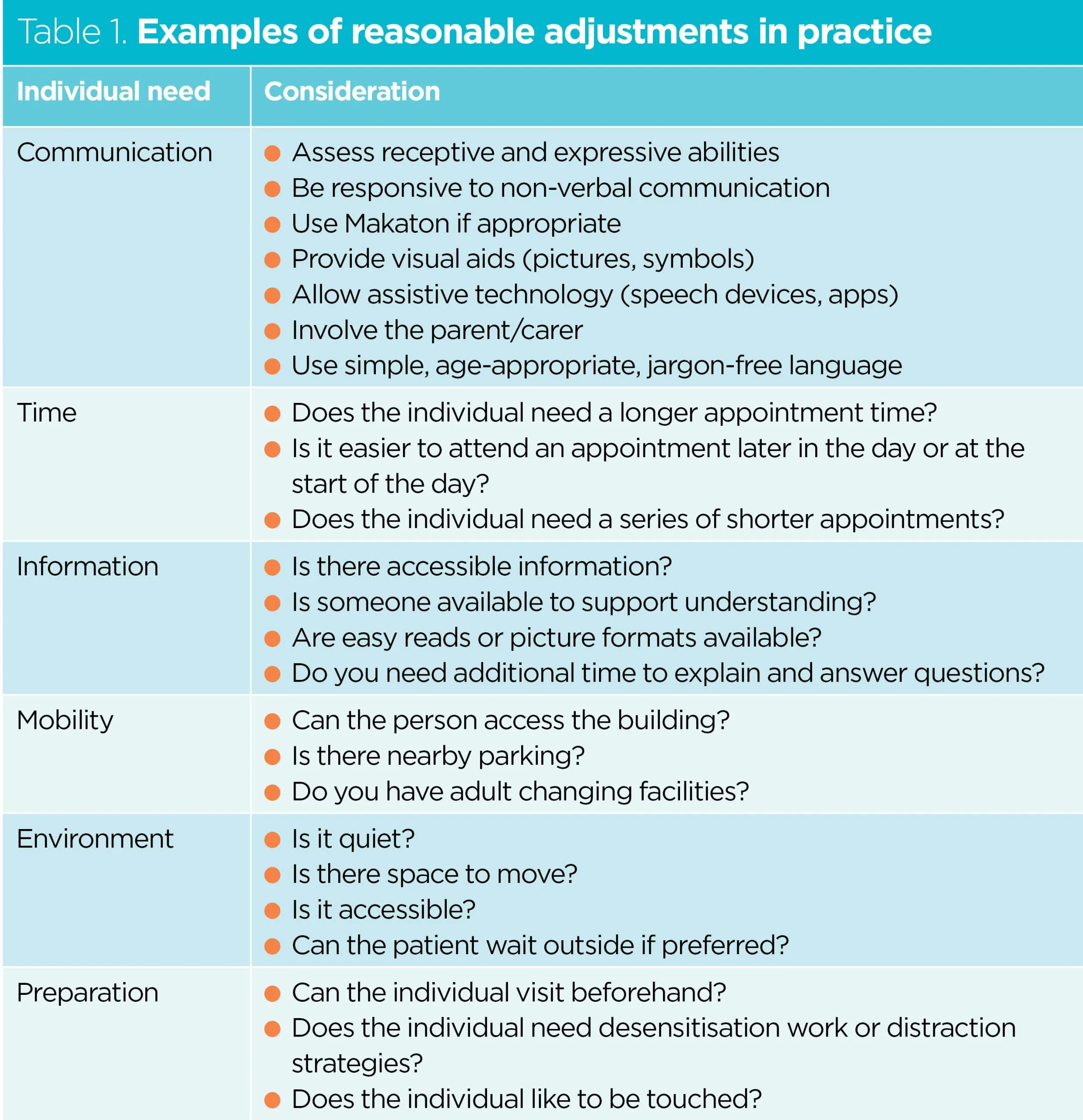
George et al (2022) discussed the benefits of implementing reasonable adjustments across the patient pathway in cancer care, and highlighted how this can improve patient experience and outcomes. Ainsworth et al (2021) discussed this issue from the perspective of lived and parental experience, and advocated the need for health professionals to embrace reasonable adjustments to help them see beyond the LD. This evidence suggests that making even the smallest adjustment can have a significant impact on the healthcare experience of an individual with LD.
Person-centred care
Autism and sensory processing issues are common in people who have LD: an estimated 50% of people with LD have an autistic spectrum condition (Mencap, no date b). A thorough assessment of the individual’s needs should be made, including how best to approach them for nursing tasks and interventions. The Public Health Agency’s (2019) Hospital Passport offers a wealth of information on person-centred need, and can support staff to:
- Establish more accurate baselines;
- Help develop better communication;
- Help with vital information, such as how pain is indicated or how medication is taken.
Clarke et al (2023) discussed an example of person-centred care for a woman with LD and autism presenting with Covid-19 during the pandemic. They explained how adhering to guidance laid out by the Equality and Human Rights Commission (2019) and adding a clause to consider the need for behavioural and emotional adjustments resulted in positive health outcomes for the woman.
Communication
Given that communication presents a challenge for many people with LD, it is vital that communication needs are assessed at the earliest opportunity. People with LD are 10 times more likely to have a visual impairment compared with the general population and are at a significantly greater risk of hearing impairments (McClimens et al, 2015). This must be considered when assessing communication needs.
Section 250 of the Health and Social Care Act 2012 outlines the need for accessible information. The quick guide (Box 3) should ensure that communication needs are identified early and information about an individual’s communication needs is shared with all relevant members of the multidisciplinary team.
Box 3. Accessible information standard
- Ask – Identify/find out what communication needs an individual might have – for example, sensory issues and hearing and/or visual impairments
- Record – Ensure this information is written down clearly and is accessible for all involved in the individual’s care. This should be recorded the same way for everyone
- Alert – Recorded needs must be highly visible
- Share – Information relating to the individual’s communication needs must be shared
- Act – Ensure the individual receives information they can understand. Provide support where necessary
Source: NHS England (2024)
Challenging behaviour should be seen as a form of communication, as it often conveys anxiety, pain or distress. In many cases, hitting out is not an intent to cause harm, but a sign that an individual is in pain, struggling to cope with the environment or struggling with the demands being placed on them (Fitzpatrick et al, 2022). Offering them an opportunity to settle alongside reasonable adjustments, such as a quieter environment and more time, can help manage this, and the inclusion of family and carers can do much to alleviate their distress and anxiety (Arrey et al, 2019).
Adhering to National Institute for Health and Care Excellence (2015) guidance on challenging behaviour and LD at ward level can promote a culture of acceptance and a willingness to make adjustments for people with LD who become overwhelmed when trying to make known their needs.
Capacity legislation and best interests
Legislation such as the Mental Capacity Act 2005 offers protection for the person with LD and supports their right to be involved in decisions about their own care. This legislation places an onus on health professionals to ensure appropriate supports are provided to help people with LD make informed decisions.
If health professionals are concerned that an individual lacks the capacity to make their own decisions, the legislation prompts the need for a mental capacity assessment. This ensures that it is the best interests of the individual, and not the assumptions of the health professionals treating them, that determine the decision-making process (Jayes et al, 2022). Jayes et al (2022) also asserted that these assessments ensure the person can be involved in advanced care planning with supports – such as family members, or a learning disability liaison nurse or speech and language therapist – to ensure their voice is heard.
Education about LD
Enhancing nurses’ understanding of the unique needs and challenges faced by individuals with intellectual disabilities through educational interventions can be a useful strategy to reduce stigma, leading to more compassionate and effective care (O’Reilly et al, 2018). O’Reilly et al (2018) and Desroches et al (2019) highlighted the importance of developing nurses’ knowledge of legislation and providing specialised training to improve nurses’ understanding of the quality of life of adults with intellectual disabilities. Furthermore, this can help address the reported lack of confidence and training to care for patients with LD identified by Cashin et al (2022).
Another approach is to include collaborative education with practitioners who are specialists in LD into continuing professional development for staff. This has been suggested as a way of demystifying LD, and alleviating staff anxieties and fears when providing care to individuals with LD – particularly in settings such as palliative or end-of-life care (Bailey et al, 2016). Furthermore, by highlighting the abilities and positive attributes of individuals with LD, these interventions can help to lower perceptions of low ability and dangerousness, thereby fostering acceptance and inclusivity (Werner and Abergel, 2018; Blundell et al, 2016).
Overall, a comprehensive approach that includes specialised training, education on legislation, collaborative learning and awareness-raising initiatives is crucial in combating stigma experienced by individuals with LD in nursing.
Conclusion
As the needs and characteristics of people with LD continue to change, driven by factors such as increased longevity and higher rates of comorbidity, it is clear that much remains to be done to meet the needs of this diverse population more effectively. Addressing stigma head-on is essential to ensuring equitable care for this population.
Nurses must recognise the enduring impact of historical stigma towards people with LD, as this gives an important context to the impact on health outcomes, and highlights the movement for greater equality and inclusion. Education is only the starting point; adherence to legislation around reasonable adjustments can create a more inclusive care environment that fully embraces a more inclusive caring culture.
- The third article in the series looks at healthcare and wellbeing inequalities in the prison setting
Key points
- Stigma towards people with learning disabilities has a significant historical background and is evident throughout healthcare
- People with learning disabilities die earlier than those in mainstream society because of stigma
- Reasonable adjustments can be made to meet the needs of people with learning disabilities
- Nurses should consider their own bias when caring for people with learning disabilities
Ailey SH et al (2015) Factors related to complications among adult patients with intellectual disabilities hospitalized at an academic medical centre. Intellectual and Developmental Disabilities; 53: 2, 114–119.
Ainsworth V et al (2021) How to get care right for people with learning disabilities in the emergency department: ask and engage. Emergency Nurse; 29: 2, 32-41.
Arrey SK et al (2019) In search of care strategies for distressed people with communication difficulties and a learning disability in palliative care settings: the lived experiences of registered learning disability nurses and palliative care professionals. Journal of Research in Nursing; 24: 6, 386–400.
Bailey M et al (2016) Surveying community nursing support for persons with an intellectual disability and palliative care needs. British Journal of Learning Disabilities; 44: 1, 24-34.
Blundell R et al (2016) The association between contact and intellectual disability literacy, causal attributions and stigma. Journal of Intellectual Disability Research; 60: 3, 218-227.
Carey IM et al (2016) Health characteristics and consultation patterns of people with intellectual disability: a cross-sectional database study in English general practice. British Journal of General Practice; 66: 645, e264-e270.
Cashin A et al (2022) A survey of Registered Nurses’ educational experiences and self-perceived capability to care for people with intellectual disability and/or autism spectrum disorder. Journal of Intellectual & Developmental Disability; 47: 3, 227–239.
Chapman M et al (2018) Improving services for people with learning disabilities and dementia: findings from a service evaluation exploring the perspectives of health and social care professionals. British Journal of Learning Disabilities; 46: 1, 33-44.
Clarke P et al (2023) Person-centred critical care for a person with learning disability and Covid-19: case study of positive risk taking. British Journal of Nursing; 32: 16, 776-784.
Daley SG, Rappolt-Schlichtmann G (2018) Stigma consciousness among adolescents with learning disabilities: considering individual experiences of being stereotyped. Learning Disability Quarterly; 41: 4, 200-212.
Desroches ML et al (2019) Nurses’ attitudes and emotions toward caring for adults with intellectual disabilities: results of a cross-sectional, correlational-predictive research study. Journal of Applied Research in Intellectual Disabilities; 32: 6, 1501-1513.
Equality and Human Rights Commission (2019) What do we mean by reasonable? qualityhumanrights.com, 19 February (accessed 30 June 2025).
Fitzpatrick R et al (2022) Improving pain-related communication in children with autism spectrum disorder and intellectual disability. Paediatric & Neonatal Pain; 4: 1, 22-32.
Foundation for People with Learning Disabilities (no date) Ageing. learningdisabilities.org.uk (accessed 25 June 2025).
George S et al (2022) Making reasonable adjustments to cancer services for people with learning disabilities. Cancer Nursing Practice; 21: 5, e1806.
Glover G et al (2020) An observational cohort study of numbers and causes of preventable general hospital admissions in people with and without intellectual disabilities in England. Journal of Intellectual Disability Research; 64: 5, 331–344.
Haft SL et al (2023) A systematic review of the consequences of stigma and stereotype threat for individuals with specific learning disabilities. Journal of Learning Disabilities; 56: 3, 193-209.
Heslop P et al (2014) The Confidential Inquiry into premature deaths of people with intellectual disabilities in the UK: a population-based study. The Lancet; 383: 9920, 889–895.
Hughes-McCormack LA et al (2018) Prevalence and general health status of people with intellectual disabilities in Scotland: a total population study. Journal of Epidemiology & Community Health; 72: 1, 78–85.
Jayes M et al (2022) Mental capacity legislation and communication disability: a cross-sectional survey exploring the impact of the Covid-19 pandemic on the provision of specialist decision-making support by UK SLTs. International Journal of Language & Communication Disorders; 57: 1, 172-181.
Lynn News (2024) Autistic boy Mattheus Ferreira Vieira, 11, of King’s Lynn died of sepsis at Queen Elizabeth Hospital that was not spotted in time, inquest hears. lynnnews.co.uk, 28 February (accessed 17 June 2025)
McCarron M et al (2015) Mortality rates in the general Irish population compared to those with an intellectual disability from 2003 to 2012. Journal of Applied Research in Intellectual Disabilities; 28: 5, 406–413.
McClimens A et al (2015) Hearing problems in the learning disability population: is anybody listening? British Journal of Learning Disabilities; 43: 3, 153-160.
Mencap (no date a) What is a learning disability? mencap.org.uk (accessed 17 June 2025).
Mencap (no date b) Autism (ASD). mencap.org.uk (accessed 17 June 2025).
Mencap (no date c) How common is learning disability in the UK? mencap.org.uk (accessed 25 June 2025).
Mencap (2012) Death by Indifference: 74 Deaths and Counting – A Progress Report 5 Years On. Mencap.
Mencap (2007) Death by Indifference: Following up the ‘Treat me Right!’ Report. Mencap.
National Institute for Health and Care Excellence (2015) Challenging Behaviour and Learning Disabilities: Prevention and Interventions for People with Learning Disabilities whose Behaviour Challenges. NICE.
NHS (2019) The NHS Long Term Plan. NHS.
NHS England (2024) The Reasonable Adjustment Digital Flag action checklist: what you need to do to achieve compliance. england.nhs.uk, 4 April (accessed 25 June 2025).
Nicholson E et al (2022) Healthcare utilisation and unmet needs in children with intellectual disability: a propensity score matching approach using longitudinal cohort data. Journal of Intellectual Disability Research; 66: 5, 442-453.
Oguntayo R et al (2020) Psychosocial factors influencing learning difficulties among individuals with special needs. European Review of Applied Sociology; 13: 20, 33-42.
O’Reilly K et al (2018) An exploration of the practice, policy and legislative issues of the specialist area of nursing people with intellectual disability: a scoping review. Nursing Inquiry; 25: 4, e12258.
Oxtoby K (2020) How unconscious bias can discriminate against patients and affect their care. BMJ; 371: m4152.
Pelleboer-Gunnink HA et al (2017) Mainstream health professionals’ stigmatising attitudes towards people with intellectual disabilities: a systematic review. Journal of Intellectual Disability Research; 61: 5, 411–434.
Public Health Agency (2019) HSC Hospital Passport and guidance notes. publichealth.hscni.net, 12 September (accessed 17 June 2025).
Richards M et al (2019) Community-based arts research for people with learning disabilities: challenging misconceptions about learning disabilities. Disability & Society; 34: 2, 204-227.
Sakellariou D, Rotarou ES (2017) Access to healthcare for men and women with disabilities in the UK: secondary analysis of cross-sectional data. BMJ Open; 7: e016614.
Scherer N et al (2023) ‘Do they ever think about people like us?’: the experiences of people with learning disabilities in England and Scotland during the Covid-19 pandemic. Critical Social Policy; 43: 3, 423-447.
Scior K, Werner S (2015) Changing Attitudes to Learning Disability: A Review of the Evidence. Mencap.
Shakespeare T et al (2017) Blaming the victim, all over again: Waddell and Aylward’s biopsychosocial (BPS) model of disability. Critical Social Policy; 37: 1, 22-41.
Tuffrey-Wijne I et al (2014) The barriers to and enablers of providing reasonably adjusted health services to people with intellectual disabilities in acute hospitals: evidence from a mixed-methods study. BMJ Open; 4: 4, e004606.
Tuffrey-Wijne I et al (2013) Identifying the factors affecting the implementation of strategies to promote a safer environment for patients with learning disabilities in NHS hospitals: a mixed-methods study. Health and Social Care Delivery Research; 1: 13.
Werner S, Abergel M (2018) What’s in a label? the stigmatizing effect of intellectual disability by any other name. Stigma and Health; 3: 4, 385-394.
White A et al (2023) LeDeR Annual Report Learning from Lives and Deaths: People with a Learning Disability and Autistic People 2022. King’s College London.
Williamson EJ et al (2021) Risks of Covid-19 hospital admission and death for people with learning disability: population based cohort study using the OpenSAFELY platform. BMJ; 374: n1592.
World Health Organization (2025) ICD-11 for mortality and morbidity statistics – 6A00 disorders of intellectual development. icd.who.int, January (accessed 25 June 2025).
link
More Stories
Preparing a “Landing Pad”: Mitigating OBBBA’s Harms to the Medicaid Safety Net
Adults with Intellectual and Developmental Disabilities Face Critical Mental Health Care Gaps, New Study Finds
Alabama Neurodevelopment Center aims to boost mental health resources in Birmingham, the state